The first time someone used the words “rejection sensitive dysphoria” in a sentence directed at me, it landed like a key turning in a lock.
I had already been called too sensitive for approximately 35 years. By teachers, by ex-partners, by a line manager who meant it kindly. By myself, on the worst nights, when I had spent four hours convinced that a two-word reply from a friend meant the friendship was ending.
I had done therapy. CBT. A short course of antidepressants for what a GP described as “mild anxiety.” None of it touched the part that was actually broken. Because none of it was aimed at the right thing.
Getting an ADHD diagnosis in my early forties, and then learning about RSD, did not fix everything. But it did something I had not expected: it made the past make sense. All of it. The friendships I had quietly self-destructed out of. The jobs I had abandoned before anyone could fire me. The years I spent performing calm while my entire nervous system was braced for impact.
For women with ADHD, RSD does not just show up — it compounds. It stacks. It arrives wearing a thousand different disguises, and it often goes unnamed for so long that by the time you finally find a word for it, the damage is already in the walls.
This article is about why. And about what actually helps.
A note before we start: This article is based on lived experience and ADHD-informed education. It is not medical advice. The research on RSD in women specifically is still limited — much of what we know comes from clinical observations and first-person accounts. If what you read here sounds like you, it is worth discussing with a professional who understands ADHD and emotional dysregulation.
Diagnosed Decades Late — and What Gets Lost in Between
The average age of ADHD diagnosis for women is significantly higher than for men. Many women are diagnosed in their thirties, forties, or fifties — after a child gets diagnosed and something clicks, after a burnout that will not resolve, after years of managing with systems that work for a while and then quietly collapse.
This diagnostic gap is not random. ADHD in women often looks different. Less hyperactivity. More inattention, more internalized. More daydreaming than disruption. The criteria used to diagnose ADHD were built largely on studies of hyperactive boys. For decades, that shaped who got referred, who got assessed, and who was told they were anxious, sensitive, disorganized, or just not trying hard enough.
Here is what goes undiagnosed for all those years: not just the attention difficulties, not just the executive function struggles — but RSD.
Because RSD without a name is just a pattern of inexplicable suffering. You do not know why a slightly flat email from your manager can ruin an entire day. You do not know why you have rehearsed a difficult conversation 400 times and still cannot make yourself have it. You do not know why certain friendships feel like standing on ice — everything fine until the moment you put your weight down and fall through.
And without a name, you find explanations that fit. You are anxious. You are difficult. You are too much. You are not enough.
Decades of those explanations leave a mark. By the time many women find their way to an ADHD diagnosis, the RSD has already shaped their careers, their relationships, and their sense of who they are allowed to be in a room.
The moment is small. One message. One silence. The ADHD brain turns it into something else entirely.
From ADHD Pearls
Free RSD Reset
When one message or moment sends your nervous system sideways.
Masking is the work ADHD women do — often automatically, often from childhood — to appear neurotypical. To seem calm when the inside is chaos. To laugh off the joke that landed like a blow. To say “I’m fine” with complete conviction while the RSD spiral is already in its third hour.
Masking and RSD are a particularly bad combination.
When you cannot show that you are affected, you cannot get support. The spiral happens entirely in private. The people around you have no idea that their three-word reply started something in you that will run until midnight. And because you are so good at hiding it, those same people sometimes say: “I had no idea you were feeling that. You seemed completely fine.”
Which makes you feel, somehow, even more alone.
Masking also means that the feedback you receive about yourself is based on a performance. The praise you get is for who you are pretending to be. The criticism lands on the real version — the one you have been carefully hiding. RSD makes that asymmetry devastating.
You spend years performing competence and calm. The praise goes to the performance. The RSD goes to the person underneath it — who has been waiting, undefended, this whole time.
The exhaustion of masking also depletes the resources that could otherwise moderate emotional responses. By the time a late afternoon RSD trigger arrives, many ADHD women are already running on empty — which is precisely when regulation is hardest. The spiral hits harder. Lasts longer. Is harder to name clearly in the moment.
Looking composed. Running at capacity. Nobody in the room can tell.
A Lifetime of Being Told You Are Too Sensitive
There is a specific kind of damage that happens when you are told, repeatedly and from a young age, that your emotional responses are wrong.
Not that the thing you are feeling is valid but intense. Not that you might benefit from some support with regulation. But that you are simply overreacting. That a reasonable person would not feel this much. That something in you is broken or deficient or embarrassing.
ADHD women hear this constantly. Because they are emotional in environments that do not expect women to be emotional in this particular way. Too tearful in professional settings. Too wounded by feedback that was “constructive.” Too thrown by a shift in someone’s tone. Too attached to outcomes that do not matter as much as they seem to matter.
The irony is that none of this is a character flaw. The RSD response is neurological. The prefrontal cortex — which in ADHD brains may have reduced capacity for emotion regulation — simply cannot dampen the signal fast enough. The pain is real. The intensity is real. The reaction is not a choice.
But if you spend 30 years being told it is a choice — or a weakness, or an attention-seeking strategy — you eventually start to believe it. And that belief shapes every relationship you have, including the one with yourself.
Learning that the sensitivity is neurological does not undo those years. But it does start to separate the reaction from the shame. Which, in my experience, is where recovery actually begins.
The body responds before the thinking part catches up. That is not weakness — it is neurology.
Hormones, Estrogen, and Why RSD Fluctuates
Something that does not get discussed nearly enough: ADHD symptoms — including emotional dysregulation and RSD — are affected by hormonal fluctuations in ways they are not for men.
Estrogen interacts with dopamine in the brain. Higher estrogen levels support dopamine function, which partly explains why some women feel sharper, more regulated, and more emotionally resilient in the first half of their cycle. In the second half, as estrogen drops, ADHD symptoms often worsen. RSD spikes. Emotional regulation becomes harder. The same situations that were manageable two weeks ago now feel impossible.
This is not imagined. Research from the National Institutes of Health has highlighted the connection between estrogen, dopamine regulation, and ADHD symptom variability in women across the menstrual cycle.
For women in perimenopause or menopause, the drop in estrogen can intensify ADHD and RSD significantly — often leading to late diagnoses in women who managed adequately before hormonal changes made their coping strategies untenable.
What this means practically: tracking your cycle alongside your RSD episodes can reveal patterns that allow you to be gentler with yourself during vulnerable windows, adjust expectations, and communicate needs more clearly to the people around you. It does not eliminate the dysphoria. But it can convert a confusing, unpredictable experience into something you can at least anticipate.
If you notice your ADHD and RSD symptoms worsening significantly around your period or during perimenopause, it is worth raising with a doctor who understands the estrogen-dopamine connection. Not all do — which means advocating for yourself, which, with RSD running, is genuinely hard. But it is worth pursuing.
How RSD Shapes Relationships for ADHD Women
RSD does not stay inside the person experiencing it. It shapes everything it touches.
In friendships, it often creates a constant, exhausting monitoring process. You track tone, response time, word choice, and emoji use. You notice what the other person did not say. You read absence as meaning. A friend who has been quiet this week is probably pulling away. A reply that was warmer than usual means something went wrong before and now they are overcompensating. The friendship becomes an ongoing interpretive exercise, and you are rarely your own most reliable narrator.
In romantic relationships, RSD can create patterns that feel to partners like unpredictability or emotional intensity. A perceived slight during an ordinary evening can shift the entire emotional register of a night. The attempt to repair can feel disproportionate to what happened. And when a partner responds with frustration rather than reassurance, the spiral deepens.
In work relationships, RSD often drives two opposing strategies: people-pleasing that becomes unsustainable, or pre-emptive withdrawal that looks like aloofness or arrogance. Both are attempts to manage the threat of rejection before it arrives. Neither works for long.
One of the most painful aspects of RSD in women is how often it is used against them. “You are too sensitive to give feedback to.” “You take everything personally.” “You are too emotionally involved.” These phrases, repeated enough, can become the architecture of how a woman understands herself — and they make it harder to advocate, to push back, to take up space in ways that are healthy and necessary.
The waiting is never just waiting. For an ADHD brain with RSD, it is an entire interrogation.
Why RSD Gets Misdiagnosed as Anxiety, Depression, or BPD
If you have spent years carrying an anxiety or depression diagnosis that never quite fit, this section might be for you.
RSD looks like anxiety from the outside. The behaviours overlap: avoidance, over-preparation, hypervigilance in social situations, difficulty relaxing. A clinician unfamiliar with RSD — and specifically with how it presents in women — will often reach for the more familiar diagnosis.
The difference, in practice, is that anxiety tends to be anticipatory. It is about what might happen. RSD is reactive — triggered by a specific perceived rejection or criticism, arriving in seconds, feeling like absolute certainty. Standard anxiety treatment (exposure, cognitive restructuring, relaxation techniques) does not reach the core of RSD. You can do exposure work all year and still be floored by a clipped reply.
RSD also gets confused with depression — partly because the aftermath of a bad RSD episode looks depressive. The withdrawal, the self-criticism, the loss of motivation. But this is situational and reactive, not pervasive in the way clinical depression is. ADHD medication, which has no first-line role in depression, can meaningfully reduce RSD for many people. That difference matters for treatment.
The misdiagnosis of BPD is more complicated. There is genuine overlap between BPD and ADHD with emotional dysregulation, and the distinction matters because the treatment differs significantly. Clinicians who are not ADHD-literate sometimes interpret RSD-driven emotional intensity as borderline features. An ADHD evaluation should always be part of the picture when emotional dysregulation is prominent, particularly in women presenting with a history of relationship difficulty and mood instability.
If you have a mental health diagnosis that explains some of your experience but not the rejection sensitivity specifically — or not the ADHD patterns that surround it — it is worth pursuing a full ADHD evaluation. Many women carry multiple diagnoses before someone finally connects the dots.
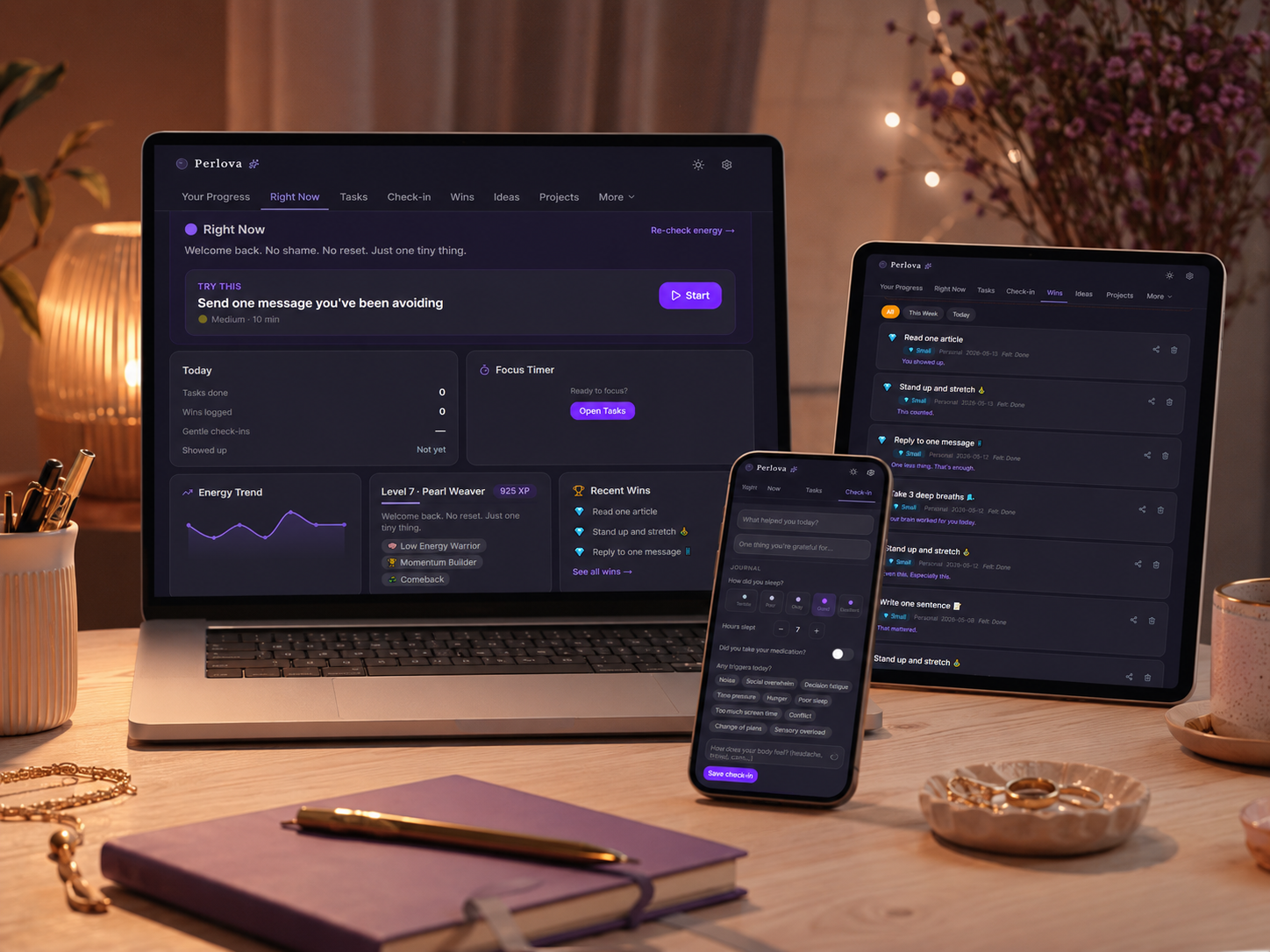
The RSD Reset: A Tool for When It Hits
Knowing the name for something does not make the moment easier. When RSD is active — when the spiral is running and the chest is tight and your brain is building a legal case against yourself — information is not what you need. You need something to do. Something small enough to be possible. Something that meets you where you actually are.
The RSD Reset is a free tool built specifically for this moment. It is not a quiz. It is not a breathing exercise that assumes you can breathe right now. It is a structured, step-by-step protocol designed around the actual intensity levels of an RSD episode — from the low-grade spiral at level three to the full shutdown at level nine or ten.
You rate how you are feeling. The tool responds with a protocol matched to that specific intensity. What to do first. What to say to yourself. How to interrupt the spiral at exactly the stage you are in, rather than offering a generic calming suggestion that assumes you are already halfway calm.
What Actually Helps With RSD as a Woman
I want to be careful here, because “what helps” lists often feel like pressure. Like more things you are supposed to be doing, and therefore more things you can fail at. That is not the intention.
What follows is what made a difference over years — not overnight, not perfectly, but meaningfully.
Getting the Right Diagnosis — and the Right Language
This is the foundation. Not because a diagnosis fixes anything, but because it changes the interpretive frame. When RSD has a name, you can stop explaining it as a personality flaw and start treating it as a neurological pattern that can be managed. The language matters. “I am too sensitive” and “I have ADHD with emotional dysregulation” lead to completely different places.
Medication (for Those for Whom It Is Appropriate)
For many women with ADHD, stimulant medication reduces the intensity and frequency of RSD episodes. Not eliminating them — but turning the volume down in ways that make regulation possible where it was not before. If you are on ADHD medication and still experiencing significant RSD, it is worth discussing whether your dose or formulation is well-matched to your current hormonal picture. Estrogen affects medication response, and many women need dose adjustments at different points in their cycle or during perimenopause.
Therapy That Understands ADHD
Standard CBT often falls short for RSD because it assumes the problem is distorted thinking that can be corrected with more accurate thinking. RSD is faster than thought. The emotional response has already concluded before rational analysis can intervene. Therapeutic approaches that work on regulation — DBT in particular — are more effective because they build skills for navigating the feeling, not just reframing it. Find a therapist who knows what RSD is. It matters more than the modality.
Naming It Out Loud — to Safe People
Telling someone you trust about RSD — before a spiral, not during one — changes the dynamic of those relationships. You do not have to manage it alone. They do not have to guess why you have gone quiet. A simple “when I go silent after something feels like rejection, this is what is happening” gives people something to work with. Not everyone will respond well. The ones who do are your actual people.
Reducing the Baseline Load
RSD is significantly worse when you are depleted. Exhausted, overwhelmed, behind on everything. Building a way of working that does not constantly put you in deficit — matching tasks to your actual energy, not your aspirational energy — reduces the overall emotional fragility that makes every RSD trigger land harder. It is not a cure. It is harm reduction. And harm reduction is worth doing.
The RSD Reset in the Moment
When the spiral has already started and the above strategies feel impossibly out of reach, the RSD Reset tool is built for exactly that moment. Rate the intensity. Follow the protocol. Do the next small thing. That is all it asks.
FAQ: RSD and ADHD Women
Is RSD more common in women with ADHD than men?
The honest answer is that we do not have large-scale research that definitively answers this. What we do know is that women with ADHD are diagnosed later, mask more, and accumulate more years of “too sensitive” feedback — all of which amplify the impact of RSD even if the underlying neurological pattern is equally prevalent. Women also face specific hormonal factors that affect dopamine regulation and therefore RSD intensity, which does not apply to men in the same way.
Can RSD be treated without medication?
Yes, though for many people medication makes a significant difference. Without medication, the most effective approach involves DBT-based skills for emotion regulation, building strong support systems with people who understand RSD, and reducing the circumstances that chronically deplete emotional reserves. Some people find that improvements in sleep, exercise consistency, and hormonal balance (in perimenopausal or menopausal women) meaningfully reduce RSD intensity even without stimulant medication. Talk to a professional who understands ADHD about what makes sense for your situation.
How do I explain RSD to someone who thinks I am just overreacting?
One framing that sometimes helps: “It is not that I think the thing that happened is a big deal. It is that my brain has a hair-trigger rejection response that fires before rational thought can get involved. I know I am overreacting. I cannot stop it in the moment. What I need is not to be told I am overreacting, but to know that you are still there.” It does not work on everyone. But it removes the question of whether the response is proportionate — which it is not, and both parties usually know it — and focuses on what actually helps.
Why does RSD feel worse in the week before my period?
Because estrogen drops in the second half of the menstrual cycle, reducing its support for dopamine function. ADHD symptoms including emotional dysregulation worsen for many women in the luteal phase (the week or two before menstruation). Tracking the timing of your worst RSD episodes alongside your cycle often reveals a clear pattern. If it is significant and consistent, it is worth discussing with a doctor or gynaecologist who understands ADHD.
I was diagnosed with anxiety years ago. Could it actually have been RSD all along?
It is possible that RSD was at the root of some of what was diagnosed as anxiety — especially if standard anxiety treatment has not fully resolved it. RSD and anxiety can also coexist. The most useful step is a full ADHD evaluation if you have not had one, and discussing with a clinician how RSD might fit into the picture. Many women find that an ADHD diagnosis — and the right support for emotional dysregulation specifically — helps in ways that anxiety treatment alone did not.
You Were Not Too Sensitive. You Were Undiagnosed.
If there is one thing I want to leave you with, it is this: the sensitivity was never the problem.
The problem was carrying it for decades without a name, without support, without anyone understanding what was actually happening in your nervous system. The problem was being told to feel less, when feeling less was never something your brain could do.
You adapted. You masked. You managed. You kept going in ways that, looking back, are actually remarkable.
And now you have a name for it. Which means you can start building something different — not a version of yourself that feels less, but a life that is better suited to the way you are wired.
On the hard days — when the RSD is running and nothing else is working — the RSD Reset tool is there. Free, no account needed, built for the exact moment when structured support matters most.
A note: This article shares personal experience and general ADHD-informed information. It is not a substitute for professional assessment, diagnosis, or treatment. If rejection sensitivity is significantly affecting your wellbeing, relationships, or safety, please speak with a qualified mental health professional.
Found this helpful? Share it with someone who gets stuck too.
For the woman who sets up the perfect system on Sunday and abandons it by Tuesday.
One short letter, every week. Real talk about ADHD, task paralysis, and the tiny wins that actually move the needle for a brain like yours. No shame. No hustle culture.